




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
General informations
Fields (28)
| Name | Label | Type | Description |
|---|---|---|---|
| Id | Medication Therapy Review ID | ID | |
| OwnerId | Owner ID | LOOKUP | |
| IsDeleted | Deleted | CHECKBOX | |
| Name | Name | AUTO NUMBER | |
| CreatedDate | Created Date | DATETIME | |
| CreatedById | Created By ID | LOOKUP | |
| LastModifiedDate | Last Modified Date | DATETIME | |
| LastModifiedById | Last Modified By ID | LOOKUP | |
| SystemModstamp | System Modstamp | DATETIME | |
| LastViewedDate | Last Viewed Date | DATETIME | |
| LastReferencedDate | Last Referenced Date | DATETIME | |
| PatientId | Account ID | MASTER-DETAIL | |
| ReviewStartDateTime | Review Start Date | DATETIME | |
| ReviewEndDateTime | Review End Date | DATETIME | |
| Status | Status | PICKLIST | |
| ConductedById | User ID | LOOKUP | |
| ReviewType | Review Type | PICKLIST | |
| ReviewSubtype | Review Subtype | PICKLIST (MULTI-SELECT) | |
| ReviewDueDateTime | Review Due Date | DATETIME | |
| Description | Description | TEXT(255) | |
| CareProgramId | Care Program ID | LOOKUP | |
| SourceSystem | Source System | TEXT(255) | |
| SourceSystemIdentifier | Source System ID | TEXT(255) | |
| SourceSysModifiedDateTime | Source System Modified Date | DATETIME | |
| SurrogateDecisionMakerId | Surrogate Decision Maker ID | LOOKUP | |
| SurrogateType | Surrogate Type | PICKLIST | |
| SurrogateLocationId | Surrogate Location ID | LOOKUP | |
| IsPatientInLtrmCareFacility | Patient in Long Term Care Facility | CHECKBOX |
Fields Details (28)
| Name | Id |
| Label | Medication Therapy Review ID |
| Type | ID |
| Required | Yes |
| Name | OwnerId |
| Label | Owner ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Required | Yes |
| Name | IsDeleted |
| Label | Deleted |
| Type | CHECKBOX |
| Required | Yes |
| Default value | false |
| Name | Name |
| Label | Name |
| Type | AUTO NUMBER |
| Required | Yes |
| Name | CreatedDate |
| Label | Created Date |
| Type | DATETIME |
| Required | Yes |
| Name | CreatedById |
| Label | Created By ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Required | Yes |
| Name | LastModifiedDate |
| Label | Last Modified Date |
| Type | DATETIME |
| Required | Yes |
| Name | LastModifiedById |
| Label | Last Modified By ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Required | Yes |
| Name | SystemModstamp |
| Label | System Modstamp |
| Type | DATETIME |
| Required | Yes |
| Name | LastViewedDate |
| Label | Last Viewed Date |
| Type | DATETIME |
| Name | LastReferencedDate |
| Label | Last Referenced Date |
| Type | DATETIME |
| Name | PatientId |
| Label | Account ID |
| Type | MASTER-DETAIL |
| Foreign key | Yes |
| Required | Yes |
| Name | ReviewStartDateTime |
| Label | Review Start Date |
| Type | DATETIME |
| Help Text | The actual date when the medication therapy review is initiated. |
| Name | ReviewEndDateTime |
| Label | Review End Date |
| Type | DATETIME |
| Help Text | The actual date when the medication therapy review is completed. |
| Name | Status |
| Label | Status |
| Type | PICKLIST |
| Picklist values | NotStarted InProgress Completed Cancelled |
| Name | ConductedById |
| Label | User ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Name | ReviewType |
| Label | Review Type |
| Type | PICKLIST |
| Picklist values | ComprehensiveMedicationReview TargetedMedicationReview |
| Name | ReviewSubtype |
| Label | Review Subtype |
| Type | PICKLIST (MULTI-SELECT) |
| Help Text | Displays the different review types of medication therapy. |
| Name | ReviewDueDateTime |
| Label | Review Due Date |
| Type | DATETIME |
| Help Text | The date when the review is expected to be completed. |
| Name | Description |
| Label | Description |
| Type | TEXT(255) |
| Name | CareProgramId |
| Label | Care Program ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Help Text | The care program associated with the medication therapy review. |
| Name | SourceSystem |
| Label | Source System |
| Type | TEXT(255) |
| Name | SourceSystemIdentifier |
| Label | Source System ID |
| Type | TEXT(255) |
| Name | SourceSysModifiedDateTime |
| Label | Source System Modified Date |
| Type | DATETIME |
| Name | SurrogateDecisionMakerId |
| Label | Surrogate Decision Maker ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Help Text | The authorized representative who attends the medication therapy review and makes healthcare related decisions on behalf of a cognitively impaired patient. |
| Name | SurrogateType |
| Label | Surrogate Type |
| Type | PICKLIST |
| Help Text | The relationship between the surrogate decision maker and the patient. |
| Picklist values | Healthcare Proxy Patient’s Guardian Patient’s Spouse Patient’s Child Patient’s Parent Patient’s Sibling Patient’s Relative Patient’s Friend Patient's Guardian of the Estate |
| Name | SurrogateLocationId |
| Label | Surrogate Location ID |
| Type | LOOKUP |
| Foreign key | Yes |
| Help Text | The address of the surrogate decision maker where the comprehensive medication review document is delivered. |
| Name | IsPatientInLtrmCareFacility |
| Label | Patient in Long Term Care Facility |
| Type | CHECKBOX |
| Required | Yes |
| Help Text | Indicates that the patient was at a long-term healthcare facility during the medication therapy review. |
| Default value | false |
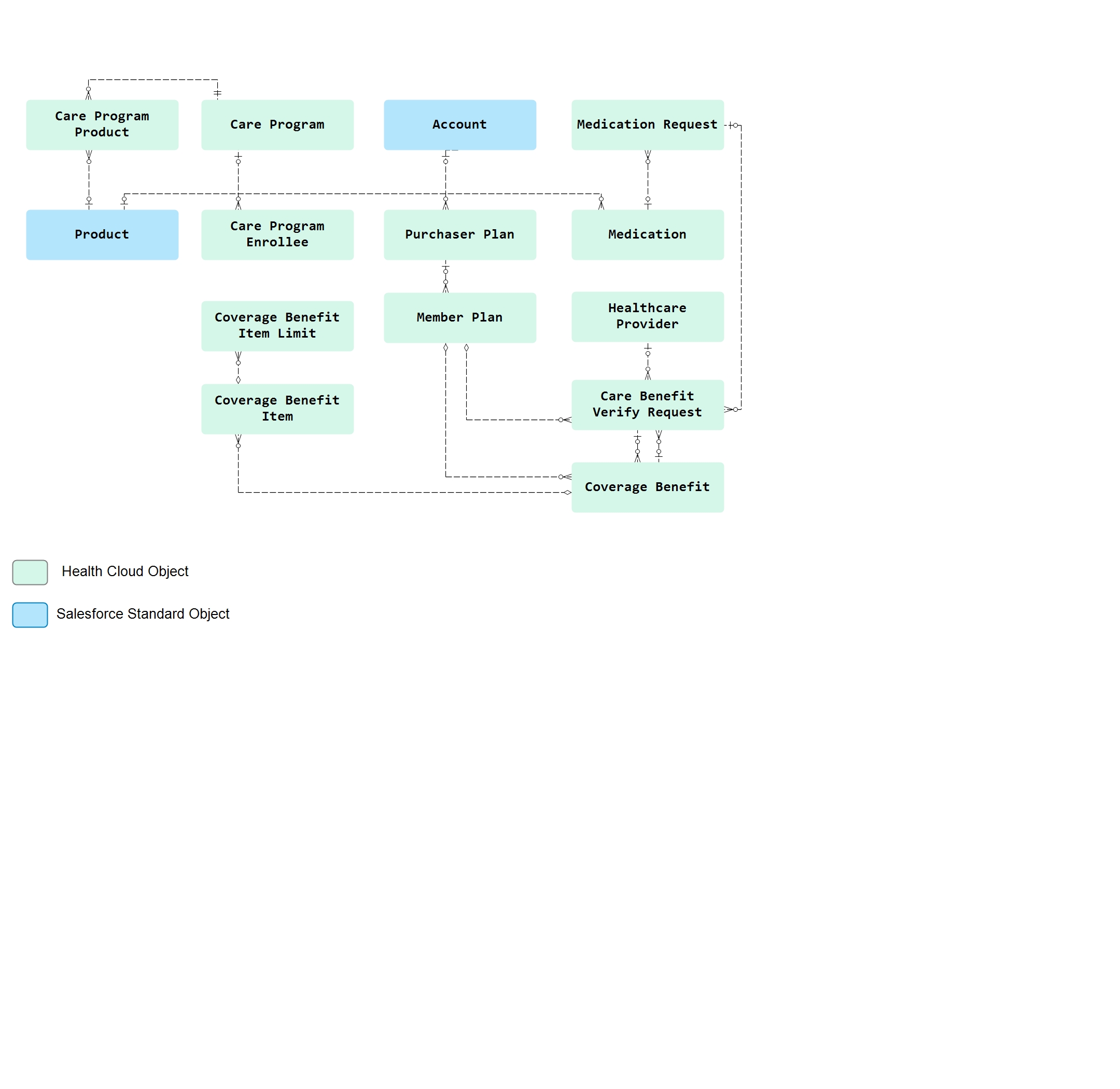
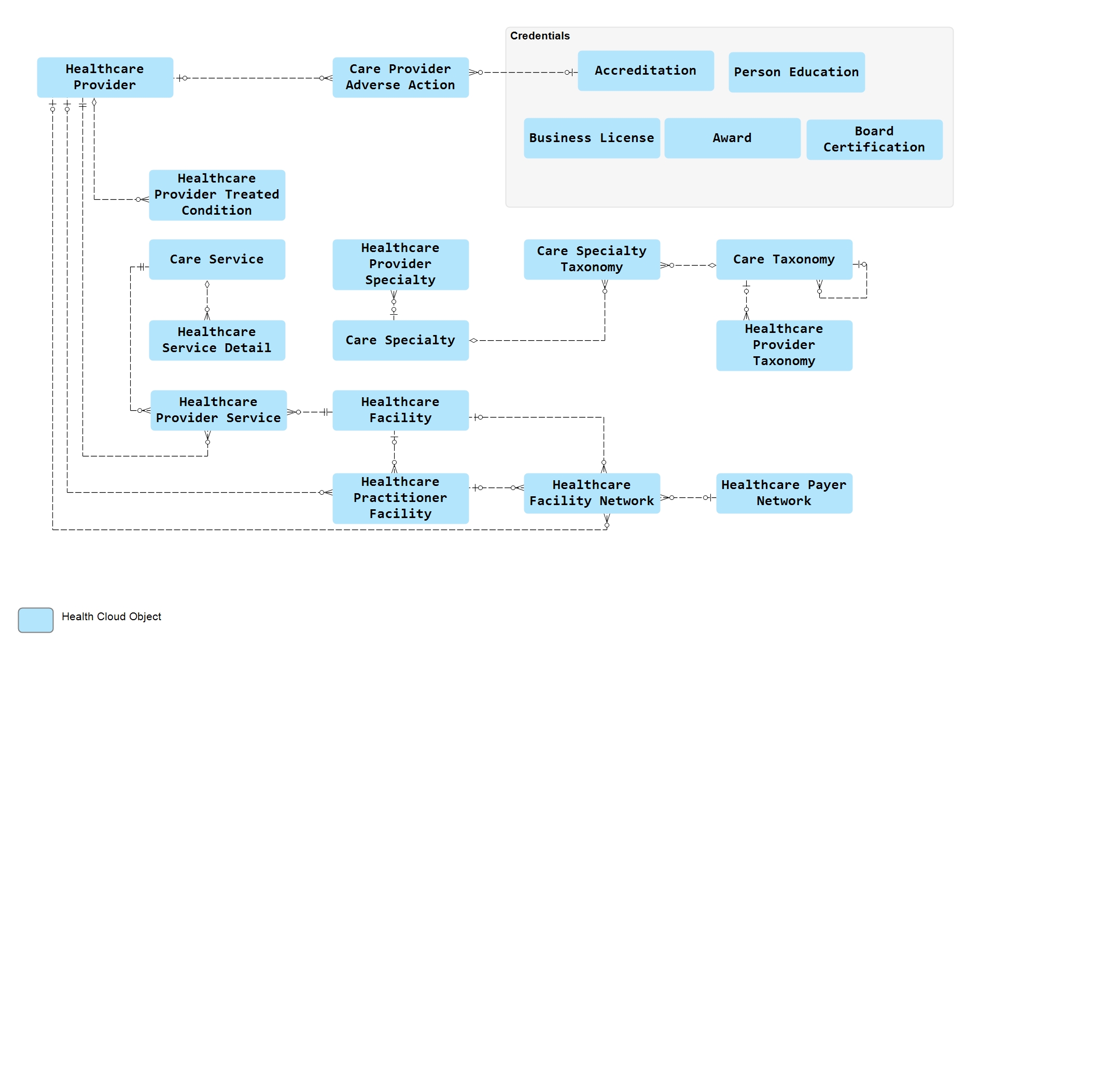
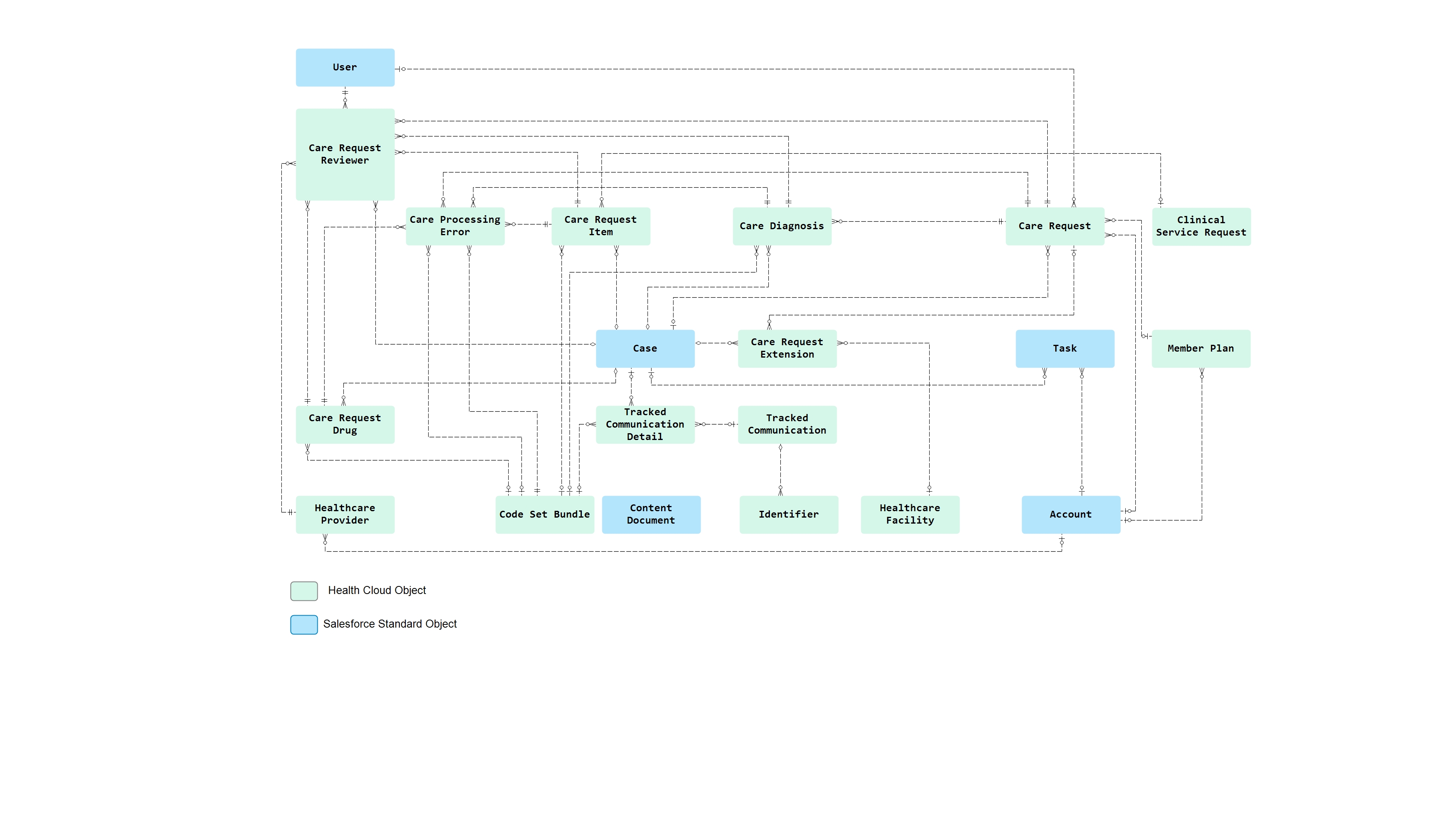
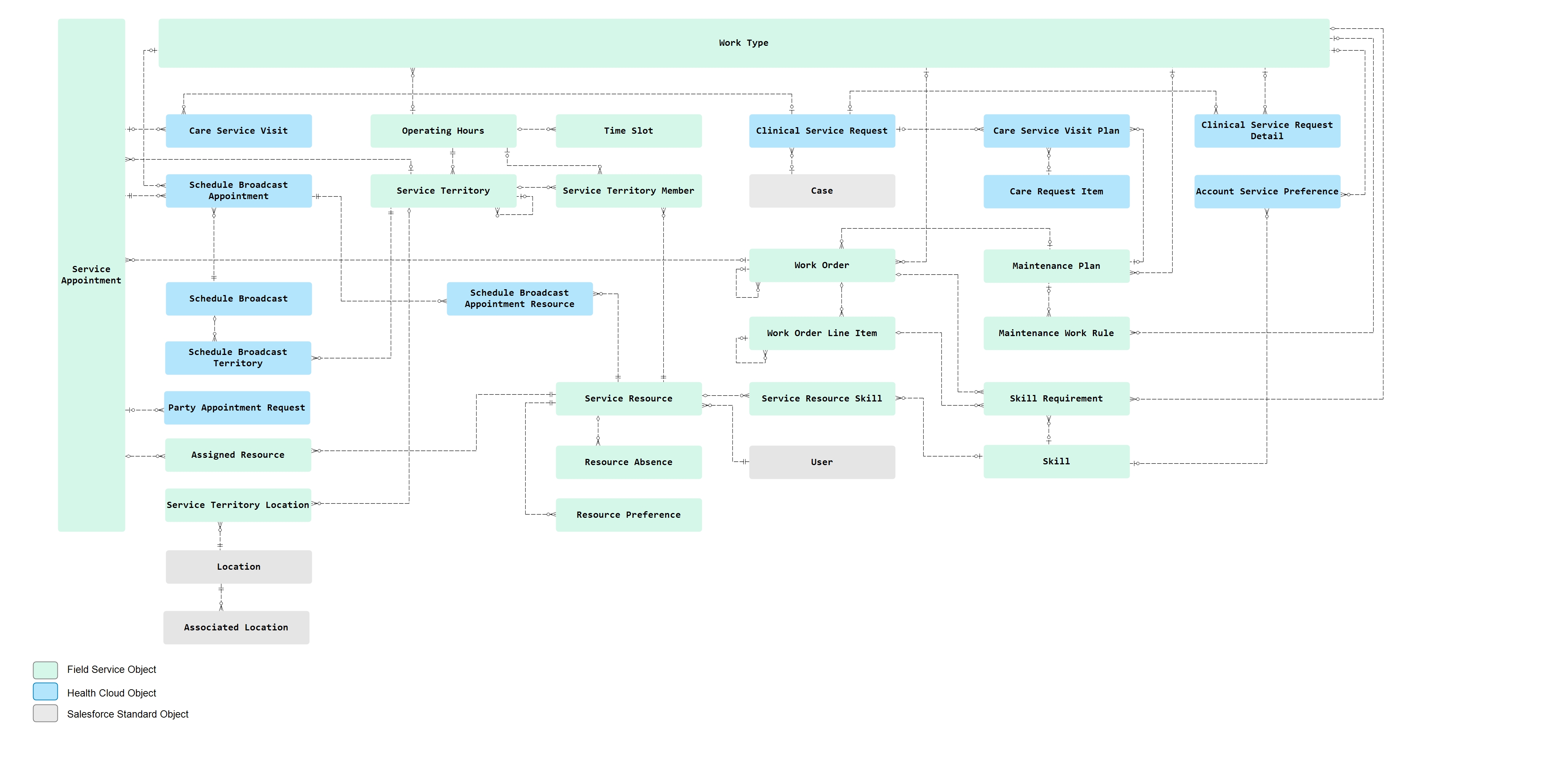
Parents relationships(14)
Children relationships(12)
Object User-defined metadata (0)
| Label | Value |
|---|